Peaceful Pill Blog

Cancel Culture gets Uncancelled with Podcast Published
Read More
Marie Fleming & Exit International Ireland
Read More

Sarco goes Viral & the Backstory
Read More
Fudging the Facts in the Azide Wars
Read More
Ensuring Northern Territory Rights Bill 2021
Read More

The Azide Wars
Read More

Suicide Related Materials Offences Act
Read More
Celebrating 25 Years since the Rights of the Terminally Ill Act
Read More

Holocaust Survivor Zsuzsi Yardley dies in Switzerland
Read More
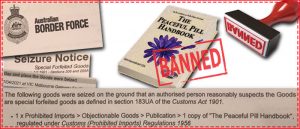
Australia Border Force Seize Peaceful Pill Handbook
Read More
July 15, 2019
Professor Avril Henry & that Infamous Police Welfare Check
It was never supposed to happen like this. A rational suicide was planned, friends (lots of friends) were told along with extended family. She thought she had her affairs in order. No one, but no one, could have predicted what happened next.
At around 9pm on Friday 15 April 2016, Professor Avril Henry had her front door smashed in by the local Exeter Police, who were followed closely by a GP, a psychiatrist and a government social worker. The ‘crisis team’ forcibly entered Avril’s house for a ‘welfare check’.
They said they had been informed by Interpol that Avril had imported Nembutal from Mexico. And they had heard she was planning to end her life. Their job, they said, was to snatch the drug from her and decide if she should be sectioned compulsorily as a psychiatric patient. To keep her from dying.
Avril’s role in this drama? An elderly woman, living alone, in a small Devon village who, with a rapidly deteriorating quality of life, had decided the trip to Switzerland was too arduous. And besides why should she?
Avril wanted to die at home and she wanted to be buried in her orchard.
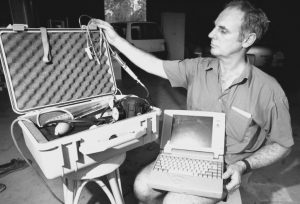
Being the highly organised person that she was, Avril took matters into her own hands. She got the Peaceful Pill eHandbook and she imported the same drug that she would have been given in Switzerland, sodium pentobarbital. That should have been the end of the matter but it wasn’t. A victimless crime to be sure.
When the police were first asked by the media what they were doing in smashing Avril’s front door down, without even ringing her front bell first, they denied they had ever been at her house.
Only on formal questioning by Avril’s lawyer was the police visit report provided. The report proved the police had attended. It proved Avril was not lying. And yes there had been a forced entry.

Professor Avril Henry & Dr Philip Nitschke, April 2016
While Avril and her friend Emma said the police took the drugs away with them, the police report states the drugs could not be found. So what is going on?
[Remember – by law, in general, you do not need to let Police into your home if they do not have a warrant. Nor do you need to tell them anything, other than your name & address]
One of the lessons from the circumstances surrounding Professor Henry’s death is the vexed question of who should be told if you are planning a rational suicide.

Avril’s door after the Police forced entry
In her own words, Avril says she would ‘talk the leg off a table’. She told anyone and everyone of her plans. Far from being ashamed of what she was planning, Avril thought the law an ass. And she thought it cruel. She wanted to make a last stand against it.
However, in telling everyone, including her internet provider company, Avril left herself open to intervention. When she told her ISP that she planned to die that night and would they please disconnect her phone and internet that day, they called for emergency help. This prompted her local GP surgery to call her with a view to dispatching immediate help to her home. Suicide prevention run amok!
As Avril said in a final email to Dr Philip Nitschke, ‘I think I had better skip lunch and get on with it’. And so she did.
Only, and to Exit’s total surprise, Avril Henry had not handed over her full stash of Nembutal when demanded by the Police several nights prior. She had kept some aside. This other stash is what she would take to end her life.

Avril Henry in conversation at her home with Philip Nitschke
Apart from the needless and senseless terrorising of Avril Henry, the element of remaining concern was the involvement of Interpol in tracing the Nembutal received by Professor Henry. In the same week as Avril Henry experienced the police raid, another UK Exit Member was also the subject of a police raid on her home. Again, the alleged tip-off came from Interpol via the Manchester Police.
More recently (July 2019) another Exit member in Australia has reported a welfare check by the Victorian Police. This elderly gent said he used Bitcoins and Protonmail to import his Nembutal. He refused the Police entry to his home. In doing so he has, presumably, retained his Nembutal bottles.
As is the way with covert police operations, Exit can only guess as to how things work but what is clear is that a Nembutal supplier or a courier company has insecure information. It is important to remember that while it may be lawful to purchase Nembutal over the counter in various Sth American countries, its importation back to one’s home country is almost always illegal.
So while you cannot blame the authorities for attempting to track down this illegal trade, it is a pity indeed that the same efforts are not made to prevent the many online scammers from robbing the elderly and vulnerable of their money.
It is the online Nembutal scammers who are the real criminals. These are the people Interpol and the Police should be out catching, rather than harassing the elderly and seriously ill who are simply trying to secure a basic end of life choice in the face of a wholly inadequate legal situation.
The experience of Professor Avril Henry is now the subject of a major, feature documentary by Vice Studios. Titled Time to Die, the film will have an advance screening in Rio Cinemas in London at 6.30pm on Wednesday 17 July 2019.
Tickets & Details at Eventbrite
June 19, 2019
Australia gets 2nd Euthanasia Law 24 Years After 1st
A quarter of a Century after the Northern Territory’s ground-breaking ROTI – Rights of the Terminally Ill Act, and the State of Victoria has finally enacted its own voluntary euthanasia law.
Touted as the world’s most conservative law for the terminally ill, the new Voluntary Assisted Dying Act of Victoria is expected to help around 150 people a year.
However to qualify for the world’s toughest law – a max security law with 68 safeguards, you need to be almost dead.
For example, Mt Martha former firefighter Troy Thornton who was slowly becoming paralysed with MSA (multiple system atrophy) was deemed ineligible.
Troy’s problem is that he would die with MSA rather than of it.
Troy’s only option was Switzerland.
The laws of all countries should do better.
With the incoming law generating all manner of questions, Exit has undertaken the first known analysis of the much-lauded ‘safeguards’ of the VAD Act. In doing so we have identified well in excess of 100 ‘safeguards’.
If you think the VAD might be something that would be useful for you at some point in the future, below are the safeguards that have been put in place to help protect you.
It is a matter of conjecture if the safeguards are help or hinder.
Exit is on the side of the latter.
Person Eligibility – Basic Requirements
- Person has decision-making capacity
- Person can understand the information relevant to the decision
- Person can retain that information
- Person must be able to use or weigh that information as part of the process of making the decision
- Person can communicate the decision
Approval Process
A person may access voluntary assisted dying if—
- the person has made a first request
- the person has been assessed as eligible by co-ordinating medical practitioner for the person
- by a consulting medical practitioner for the person
- the person has made a written declaration;
- the person has made a final request to the co-ordinating medical practitioner
- the person has appointed a contact person
- the co-ordinating medical practitioner has certified in a final review form
- the person is the subject of a voluntary assisted dying permit
Rules for Doctors – General
- A registered health practitioner may not initiate discussion with that person that is in substance about voluntary assisted dying
- A registered health practitioner must not suggest voluntary assisted dying to that person
Eligibility
- Person must be aged 18 years or more
- Person must be an Australian citizen or permanent resident
- Person must ordinarily resident in Victoria
- At the time of making a first request, have been ordinarily resident in Victoria for at least 12 months
- Person must be diagnosed with an incurable disease, illness or medical condition
- Person must be diagnosed with a disease, illness or medical condition that is advanced, progressive and will cause death
- Person must be diagnosed with a disease, illness or medical condition that is expected to cause death within weeks or months, not exceeding 6 months
- Person must be diagnosed with a disease, illness or medical condition that is causing suffering to the person that cannot be relieved in a manner that the person considers tolerable
- Person is not eligible for access to VAD only because the person is diagnosed with a mental illness
- Person is not eligible for access to voluntary assisted dying only because the person has a disability
- Person must be diagnosed with a neurodegenerative disease, illness or medical condition that is expected to cause death within weeks or months, not exceeding 12 months
Doctor Regulations
- Doctor must hold a fellowship with a specialist medical college
- Doctor must be a vocationally registered general practitioner
- Doctor must have practised as a registered medical practitioner for at least 5 years after completing a fellowship
- Doctor must have relevant expertise and experience in the disease, illness or medical condition expected to cause the death of the person
Person Requirements
- Person may make a first request
- Request must be clear and unambiguous
- Request made personally
- Person may decide at any time not to continue
- Process ends if a person decides not to continue
- Within 7 days after receiving a first request from a person, the registered medical practitioner – accepts the first reques
- Within 7 days after receiving a first request from a person, the registered medical practitioner – refuses the first request
- If first request accepted, practitioner must record his/ her acceptance in the person’s medical record
- If first request accepted, practitioner must record patient’s request in the person’s medical record
- The co-ordinating medical practitioner must not commence the first assessment unless the practitioner has completed approved assessment training
- If co-ordinating medical practitioner is unable to determine whether the person has decision-making capacity they must refer the person to a registered health practitioner who has appropriate skills and training
Specialists
- If the co-ordinating medical practitioner is unable to determine whether the person’s disease, illness or medical condition, co-ordinating medical practitioner must refer the person to a specialist registered medical practitioner who has appropriate skills and training in that disease
- Specialist must determine status
- Specialist must provide clinical report
Neurological Specialists
- If the co-ordinating medical practitioner is able to determine that the person has a disease, illness or medical condition that is neurodegenerative, and will cause death within 12 months, co-ordinating medical practitioner must refer the person to a specialist registered medical practitioner who has appropriate skills and training in that particular disease, illness or medical condition
- Specialist must determine status
- Specialist must provide a clinical report
- Coordinator practitioner must adopt specialist’s report
Coordinating Practitioner
- If coordinating practitioner assesses person as eligible they must inform patient of: person’s diagnosis and prognosis
- If coordinating practitioner assesses person as eligible they must inform person of: treatment options and likely outcomes
- If coordinating practitioner assesses person as eligible they must inform patient of: palliative care option and likely outcomes
- If coordinating practitioner assesses person as eligible they must inform patient of: potential risks of taking a poison or controlled substance or a drug of dependence
- If coordinating practitioner assesses person as eligible they must inform patient of: expected outcome of taking a poison or controlled substance or a drug of dependence
- If coordinating practitioner assesses person as eligible they must with patient’s consent, inform the family of all relevant clinical guidelines
- If coordinating practitioner assesses person as eligible they must with patient’s consent, inform the family of plan in respect of the self-administration of a voluntary assisted dying substance
- Coordinating practitioner must assess person for meets all the eligibility criteria
- Coordinating practitioner must assess person understands the information
- Coordinating practitioner must assess person acting voluntarily and without coercion
- Coordinating practitioner must assess person’s request is enduring
- If deemed eligible by coordinating practitioner, he / she must refer the person to another registered medical practitioner for a consulting assessment
- Consulting medical practitioner must not commence a consulting assessment unless the practitioner has completed approved assessment training
Written Declarations
- Declaration must be witnessed by an eligible person over 18 (not a beneficiary of the will/ owner of the hospice where person is being treated or providing health care)
Final request
- Can only make final request if made written declaration
- Final request must be to coordinating practitioner by person personally
- Final request must be made at least 9 days after 1st request
- Final request must be made at least one day after deemed eligible by practitioners
Contact Person
- Person must appoint a contact person
- Must use the right form
- Person must appoint a contact person in presence of a witness
- Witness must sign form
Final Review
- Coordinating practitioner must undertake a final review
- Must review all forms
- Complete a final review form
- Certify the request and assessment process has been completed as required by this Act
- Co-ordinating medical practitioner must give the VAD Review Board a copy of the completed final review form, and copies of all other forms within 7 days after completing the final review form
- Coordinating practitioner must certify in final review form that request and assessment process has been completed as required by this Act
- Coordinating practitioner can then apply for VAD permit
Self-administration permit
- A self-administration permit – enables coordinating practitioner to prescribe and supply the voluntary assisted dying substance that the person can self-administer or obtain, possess, store, use
- Coordinating practitioner must be satisfied person is physically incapable of the self-administration or digestion
- Coordinating practitioner must be satisfied person has decision-making capacity
- Coordinating practitioner must be satisfied person’s request is enduring
Practitioner administration permit
- A practitioner administration permit – allows coordinating practitioner to prescribe and supply to the person a sufficient dose
- possess, use, and administer in the presence of a witness to the person if person is physically incapable of the self-administration or digestion
- A practitioner administration permit must be on the correct form
- A practitioner administration permit must identify the person
- A practitioner administration permit be accompanied by final review form
- A practitioner administration permit be accompanied by all other forms
- A practitioner administration permit be accompanied by statement of eligibility
- A practitioner administration permit specify the poison or controlled substance or the drug of dependence
- A practitioner administration permit specify the contact person in charge of returning unused portions to the chemist
- Person must have made administration request personally
- Person must have made administration request in front of witness
- Person must have decision making capacity
- Person’s request for VAD is enduring
- Person must understand that substance is to be administered immediately after the request
Requirements of Pharmacist
- Pharmacist must destroy returned portion as soon as practicable
- Pharmacist must record and notify VAD Review Board of disposal within 7 days
- Harsh penalties for misuse, trafficking etc of drug offences
Role of Secretary (Head of the Department of Health and Human Services)
- VAD Permits are determined by Secretary
- Secretary may refuse if not satisfied with request and assessment process
- VAD permit must be on prescribed form
Storage of VAD substance
- VAD substance must be stored in a locked box
- Package/ container must have warning label
- Package/ container label must state the dangers of self-administering substance
- Package/ container label must state that the substance must be stored in a locked box
- Package/ container label must state that any unused or substance must be returned to pharmacist at the dispensing pharmacy
Harsh Criminal Penalties for Non Compliance
- Penalty of life imprisonment if another person administers what is provided under a self-administration permit
- Penalty of 5 years imprisonment if another person induces a person to request VAD
- Penalty of 5 years imprisonment if another person induces a person to self-administer substance
- Penalty of 5 years imprisonment if any forms are falsified:
- a first assessment report form
- a consulting assessment report form
- a written declaration
- a contact person appointment form
- a final review form
- a VAD substance dispensing form
- a VAD substance disposal form
- a co-ordinating medical practitioner administration form
- Penalty of 12 months imprisonment if contact person fails to return unused drugs to pharmacy within 15 days after death
- 60 penalty points for failure to provide Board with paperwork
- Criminal liability for officers of body corporate who fail in due diligence
- VAD Review Board – with wide-ranging powers of oversight and compliance
June 15, 2019
Correction to Derek Humphry Assisted Suicide History Chronology
This week the Godfather of the Assisted Suicide movement, Derek Humphry, made an unfortunate, but significant, omission in his chronology of the history of Assisted Suicide laws up to and including June 2019.
Exit is certain that this was nothing more than a sleight of the pencil, but in these days of ‘alternative facts’, the truth matters more than ever!
Correction to Derek Humphry’s Chronology
The first place in the world to allow a doctor to administer a legal, lethal, voluntary injection to a patient was the Northern Territory of Australia.
The Rights of the Terminally Ill Act was conceived and presented to the Northern Territory by then Chief Minister, Marshall Perron. The ROTI Act was enacted 1 July 1996.
The doctor who administered the first legal, lethal, voluntary injection (to patient Bob Dent (who was suffering from prostate cancer) was Exit International Founder & Director, Dr Philip Nitschke.
The Rights of the Terminally Ill Act lasted only nine months before it was overturned by the Euthanasia Laws Act in the Australian Federal Parliament. This Act became known as the Kevin Andrews Act (named after the conservative catholic politician from Melbourne who presented the Private Member’s bill to the Parliament).
The law was able to be overturned thanks to Section 122 of the Australian Constitution. This historical quirk allows the Federal Parliament to make laws for the three territories of Australia. This Section does not apply to the States of Australia.
In his email blog on 14 June, Derek wrote:
‘Various forms of medical assisted dying have been approved in the following states and nations. Each law has its own limits, rules and guidelines. All but Switzerland forbid foreigners this type of help to die. Only Canada, the Netherlands, Colombia and Belgium permit chosen death via doctor lethal injection as well as oral ingestion; all others are by doctor prescription which the patient drinks. A policy statement in England gives clear guidance when helping another to die would not be prosecuted, but there is no law.’

Sydney Morning Herald – 1 July 1996 (click on image to enlarge)
Corrected Historical Chronology
- Switzerland 1940
- Northern Territory of Australia (1 July 1996 – 27 March 1997)
- *Oregon (passed in 1994 but not enacted until late 1997)
- Colombia l997
- The Netherlands 2002
- Belgium 2002
- *Washington 2008
- Luxembourg 2009Montana 2009 (court ruling only)
- England & Wales 2010 (prosecution policy statement only. No law.)*Vermont 2014
- Quebec 2015
- *California 2016
- Canada 2016
- *Colorado 2016
- Washington DC 2017
- *Hawaii 2019
- *New Jersey 2019
- Victoria (Australia) 2019
- *Maine (2019)
The 9 US states are starred*:
June 5, 2019
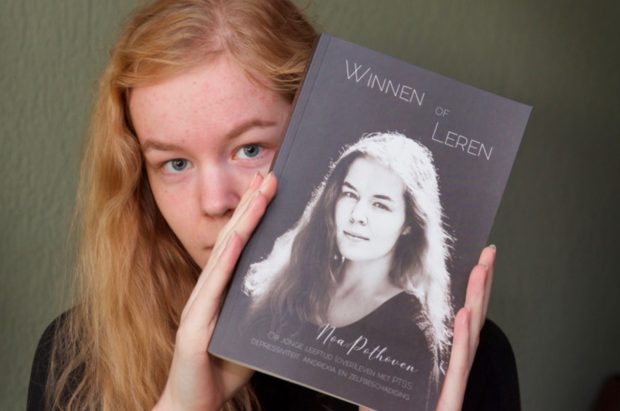
The Death of Noa Pothoven
5 June 2019
I guess it was bound to happen.
An attractive young Dutch girl would be given euthanasia. Or would she?
The furor that has erupted over the death of 17-year old Noa Pothoven was fake news waiting to happen.
Here was a girl who was raped and abused and who said she could not and never would get over it. Her book Winning or Learning was a brave move to explain her headspace.
Noa said she was breathing but not living. Her PTSD, anorexia, depression had gotten the better of her. In an interview before her death she was hopeful that ECT might break the cycle of negativity. This proved not to be the case.
She had approached the Levenseindekliniek in The Hague for help. Despite what media reports have said, they turned her down.
Talk about a hot potato!
Especially after the controversial suicide of Ximena Knol, the Dutch 19 year old who allegedly took Middel X to suicide in February 2018.
Her parents are still baying for blood from Dutch group, CLW whom they (wrongly) hold responsible.
And so it was that Noa stopped eating and drinking. Her parents agreed that she would not be forcibly sent to hospital and force-fed (unlike before).
This is how Noa died.
She was not euthanized.
Despite such credible news outlets such as Euronews and The Independent getting it so wrong, so did Exit get it wrong.
We, too, thought this was an example of progressive Dutch liberalism. We were (and are) proud to call this country home.
While the Daily Mail and the other UK tabloids were horrified at the news, Exit warmly welcomed that the Dutch were prepared to acknowledge the suffering of a 17-year old with psychiatric illness.
We wondered about her parents, in their supportive role. In a taped interview in Dutch before Noa’s death, they were only just holding it together. They said they remained hopeful.
Their bravery in allowing their daughter to choose to die should not be overlooked.
And this ties in with how we made our point about our support for Noa’s right to decide.
And we sat back and thought about how her situation is a far cry from the 63 safeguards that have been built into the forthcoming Australian (State of Victoria) assisted dying legislation.
Super safe legislation = unworkable legislation as the Canadians for one are now discovering.
In Melbourne, you will need to be almost dead just to qualify. Just ask Troy Thornton.
He was becoming slowly paralyzed but even that didn’t make him sick enough to use the Victorian law.
The point is that the Dutch allow for psychiatric suffering. So do the Belgians.
The Swiss do on occasion. In all cases the person must have mental capacity.
As if to restate the obvious, just because you are depressed this does not mean you have lost capacity. Far from it.
There is something about the Netherlands that makes the fake news of how Noa died not that relevant.
While the English-speaking world can eat humble pie in that a 17-year old girl was not ‘put down’ by the Dutch State, the fact that her parents allowed her to go through with her wishes, and that the medical profession (in hero role) did not rush in demanding she be saved from herself, says something about this place.
The type of respect shown to Noa, if not by not helping her, then at least by not interfering, is a good lesson to those countries who insist on ‘nanny-stating’ the rest of us to death … so to speak.
Rational suicide is a fundamental human right. That is why it is not illegal!
Noa’s Instagram handle was @noamaestro The page has since been disabled by Instagram.
Her last post read:
A sad last post. I doubted for a long time whether I would share it here, but I decided to do it anyway. Maybe it is unexpected because of my posts about the recording, but my plan had been there for a long time so it is not impulsive.I get straight to the point: within a maximum of 10 days I will die. After years of fighting and fighting it is finished. I have now stopped eating and drinking for a while, and after many conversations and reviews it has been decided that I will be released because my suffering is unbearable. It’s finished. I have not really been alive for so long, I survive, and not even that. I am still breathing but I am no longer alive.I am well cared for, I get strong pain relief and am with my family all day (I am in a hospital bed in the living room). I’m saying goodbye to the most important people in my life.I can no longer call and I can barely app. If I do not approach you myself then it will no longer be possible to say goodbye, I am very weak so limit this to the most important people. I hereby also ask if you do not want to spam me with pleas or this is possible, I can no longer handle this.It’s fine this way. Do not convince me that this is not good, this is my decision and it is final. Love is letting go, in this case … ❤Thanks for your support always. It’s fine this way. It will be posted here in a while when I die, so that will become clear.Love from No
Exit